Fallen Arches What You Need
Overview

Of the many body parts we benignly neglect, our feet may be the most taken for granted. They get us where we need to go, supporting a lot of weight given their size relative to the rest of our bodies. They are structurally complex, comprising 26 bones, 33 joints, and 100+ muscles, tendons, and ligaments apiece. Indeed, over a quarter of the bones in the body are located in the feet. Most human feet have arches much like the ones in some bridges and other architectural structures. And much like these man-made structures, our bipedal arch turns out to be a useful engineering phenomenon. ?The arches distribute weight evenly across the feet and up the legs, and can affect walking. A well-developed arch is balanced between rigidity (for stability and flexibility (for adapting to surfaces). What, then, are the implications of fallen arches, otherwise known as flat feet, where no or little foot arch exists and the instep of the foot touches the ground? There are two types of flat feet. A person with flexible flat feet has some arch, especially when standing on the toes. A person with rigid flat feet has no arch whatsoever. Infants usually have flat feet, with the arch developing in childhood.
Causes
Just as there are many different causes of flat feet, there are also many different treatment options. The most important aspect of treatment is determining the exact type or underlying cause of flat feet that you have. Foot and ankle specialists can determine this through thorough clinical examination and special imaging studies (e.g., x-rays, computed tomography, and/or magnetic resonance imaging). Conservative treatment is effective in the vast majority of flat foot cases, and consists of things such as insoles, splints, manipulation, or casting. Surgery is required much less frequently, and is reserved only for some of the severe types of flat foot that do not respond to conservative therapy. You may have noticed that one common element in the conservative treatment of all types of flat feet is orthoses. Many companies now manufacture semi-custom orthotic devices that not only improve comfort, but also seek to control abnormal motion of the foot. These over-the-counter inserts, in the $25 to $50 range, are an economical treatment that may help a majority of people. Unfortunately, these semi-custom devices will not fit everyone perfectly, and those of us who differ too much from the average may respond better to custom orthotic devices. Custom inserts are prescribed by your foot and ankle specialist and are made individually from either a physical or computerized impression of your feet. The only drawback of custom orthoses is their cost, ranging anywhere from $300 to $500. Many physicians recommend trying over-the-counter inserts first (and even keep them in stock) as they may save their patients large sums of money.
Symptoms
Arches can be seen as ?rolling downward? or collapsing when walking. Pain may present in lower back, hips or knees. Pain may be present on the bottom of the heels, within the arch, within the ankles or even the forefoot. Swelling can occur. Pain may occur in the anterior leg muscles.
Diagnosis
You can test yourself to see if you have flat feet or fallen arches by using a simple home experiment. First, dip your feet in water. Then step on a hard flat surface, like a dry floor or a piece of paper on the floor, where your footprints will show. Step away and examine your foot prints. If you see complete/full imprints of your feet on the floor, you may have fallen arches. However, it?s important to seek a second option from a podiatrist if you suspect you have fallen arches so they can properly diagnose and treat you.
pes cavus
Non Surgical Treatment
The simplest form of treatment is the use of custom fitted orthotics. For this, it is best to see a podiatrist, who is a trained medical professional that assesses feet and gives you a prescription for the orthotic. If the orthotics do not work - or if the deformity is very severe - then surgical management may be needed. There is a very wide range of procedures available, with varying downtimes and complexity. The simplest procedure of all is a simple calf release. This can be done at the back of the knee or the calf, and has a very quick recovery. It is a day-surgery procedure, and the patient can walk immediately after the surgery without the need for a cast. Recovery back to jogging can be as early as three weeks. The calf release stops the deforming force but obviously does not correct the arch itself. It is usually done in combination with some of the other procedures mentioned below. Done by itself, the patient will probably still require orthotics but by releasing the calf, it allows the orthotics to be much more effective. The other end of the spectrum is a complete reconstruction of the arch with bone work and screws to fuse joints.
Surgical Treatment

Generally one of the following procedures is used to surgically repair a flat foot or fallen arch. Arthrodesis. One or more of your bones in the foot or ankle are fused together. Osteotomy. Correcting alignment by cutting and reshaping a bone. Excision. Removing a bone or a bone spur. Synovectomy. Cleaning the sheath that covers the tendon. Tendon transfer. Using a piece of one tendon to lengthen or replace another. Arthroereisis. placing a small device in the subtalar joint to limit motion. For most people, treatment is successful, regardless of the cause, although the cause does does play a major role in determining your prognosis. Some causes do not need treatment, while others require a surgical fix.
Prevention
Donning a first-rate pair of arch supports, therapeutic socks and proper footwear before heading out to enjoy hours of holiday fun is one option to consider. Your podiatrist can help you find just the right ones. Once you have them on, they?ll help ease the amount of pressure being put on your body and keep the blood flowing in the right direction. While you?re standing in line, consider doing a bit of exercise as well. We?re not talking about channeling your inner Jack LaLanne here. Otherwise, you might attract the attention of the mall security guards. Simple ankle rotations and walking in place may help to reduce edema and give your flat feet a bit of a break. If you happen to be in a shopping mall or center where foot massages are available, take advantage of them periodically. They are likely to make you feel better and it?s a great excuse to carve out a few quiet moments for yourself. If you can?t visit a professional, tuck a personal foot massager into your purse. That way, you can lightly massage your own feet during the car ride home. Lastly, there are certain foods and nutritional supplements available that may reduce edema caused by standing on flat feet for hours at a time. The list includes potassium rich foods like raisins, bananas, baby carrots, nuts and yogurt. So, you may want to pack a snack for those trips to the mall or hit the food court before you hit the stores.
Of the many body parts we benignly neglect, our feet may be the most taken for granted. They get us where we need to go, supporting a lot of weight given their size relative to the rest of our bodies. They are structurally complex, comprising 26 bones, 33 joints, and 100+ muscles, tendons, and ligaments apiece. Indeed, over a quarter of the bones in the body are located in the feet. Most human feet have arches much like the ones in some bridges and other architectural structures. And much like these man-made structures, our bipedal arch turns out to be a useful engineering phenomenon. ?The arches distribute weight evenly across the feet and up the legs, and can affect walking. A well-developed arch is balanced between rigidity (for stability and flexibility (for adapting to surfaces). What, then, are the implications of fallen arches, otherwise known as flat feet, where no or little foot arch exists and the instep of the foot touches the ground? There are two types of flat feet. A person with flexible flat feet has some arch, especially when standing on the toes. A person with rigid flat feet has no arch whatsoever. Infants usually have flat feet, with the arch developing in childhood.
Causes
Just as there are many different causes of flat feet, there are also many different treatment options. The most important aspect of treatment is determining the exact type or underlying cause of flat feet that you have. Foot and ankle specialists can determine this through thorough clinical examination and special imaging studies (e.g., x-rays, computed tomography, and/or magnetic resonance imaging). Conservative treatment is effective in the vast majority of flat foot cases, and consists of things such as insoles, splints, manipulation, or casting. Surgery is required much less frequently, and is reserved only for some of the severe types of flat foot that do not respond to conservative therapy. You may have noticed that one common element in the conservative treatment of all types of flat feet is orthoses. Many companies now manufacture semi-custom orthotic devices that not only improve comfort, but also seek to control abnormal motion of the foot. These over-the-counter inserts, in the $25 to $50 range, are an economical treatment that may help a majority of people. Unfortunately, these semi-custom devices will not fit everyone perfectly, and those of us who differ too much from the average may respond better to custom orthotic devices. Custom inserts are prescribed by your foot and ankle specialist and are made individually from either a physical or computerized impression of your feet. The only drawback of custom orthoses is their cost, ranging anywhere from $300 to $500. Many physicians recommend trying over-the-counter inserts first (and even keep them in stock) as they may save their patients large sums of money.
Symptoms
Arches can be seen as ?rolling downward? or collapsing when walking. Pain may present in lower back, hips or knees. Pain may be present on the bottom of the heels, within the arch, within the ankles or even the forefoot. Swelling can occur. Pain may occur in the anterior leg muscles.
Diagnosis
You can test yourself to see if you have flat feet or fallen arches by using a simple home experiment. First, dip your feet in water. Then step on a hard flat surface, like a dry floor or a piece of paper on the floor, where your footprints will show. Step away and examine your foot prints. If you see complete/full imprints of your feet on the floor, you may have fallen arches. However, it?s important to seek a second option from a podiatrist if you suspect you have fallen arches so they can properly diagnose and treat you.
pes cavus
Non Surgical Treatment
The simplest form of treatment is the use of custom fitted orthotics. For this, it is best to see a podiatrist, who is a trained medical professional that assesses feet and gives you a prescription for the orthotic. If the orthotics do not work - or if the deformity is very severe - then surgical management may be needed. There is a very wide range of procedures available, with varying downtimes and complexity. The simplest procedure of all is a simple calf release. This can be done at the back of the knee or the calf, and has a very quick recovery. It is a day-surgery procedure, and the patient can walk immediately after the surgery without the need for a cast. Recovery back to jogging can be as early as three weeks. The calf release stops the deforming force but obviously does not correct the arch itself. It is usually done in combination with some of the other procedures mentioned below. Done by itself, the patient will probably still require orthotics but by releasing the calf, it allows the orthotics to be much more effective. The other end of the spectrum is a complete reconstruction of the arch with bone work and screws to fuse joints.
Surgical Treatment
Generally one of the following procedures is used to surgically repair a flat foot or fallen arch. Arthrodesis. One or more of your bones in the foot or ankle are fused together. Osteotomy. Correcting alignment by cutting and reshaping a bone. Excision. Removing a bone or a bone spur. Synovectomy. Cleaning the sheath that covers the tendon. Tendon transfer. Using a piece of one tendon to lengthen or replace another. Arthroereisis. placing a small device in the subtalar joint to limit motion. For most people, treatment is successful, regardless of the cause, although the cause does does play a major role in determining your prognosis. Some causes do not need treatment, while others require a surgical fix.
Prevention
Donning a first-rate pair of arch supports, therapeutic socks and proper footwear before heading out to enjoy hours of holiday fun is one option to consider. Your podiatrist can help you find just the right ones. Once you have them on, they?ll help ease the amount of pressure being put on your body and keep the blood flowing in the right direction. While you?re standing in line, consider doing a bit of exercise as well. We?re not talking about channeling your inner Jack LaLanne here. Otherwise, you might attract the attention of the mall security guards. Simple ankle rotations and walking in place may help to reduce edema and give your flat feet a bit of a break. If you happen to be in a shopping mall or center where foot massages are available, take advantage of them periodically. They are likely to make you feel better and it?s a great excuse to carve out a few quiet moments for yourself. If you can?t visit a professional, tuck a personal foot massager into your purse. That way, you can lightly massage your own feet during the car ride home. Lastly, there are certain foods and nutritional supplements available that may reduce edema caused by standing on flat feet for hours at a time. The list includes potassium rich foods like raisins, bananas, baby carrots, nuts and yogurt. So, you may want to pack a snack for those trips to the mall or hit the food court before you hit the stores.
All The Things You Should Understand About Heel Pain And Discomfort
Overview

Heel pain is most often caused by plantar fasciitis, a condition that is sometimes also called heel spur syndrome when a spur is present. Heel pain may also be due to other causes, such as a stress fracture, tendonitis, arthritis, nerve irritation, or, rarely, a cyst. Because there are several potential causes, it is important to have heel pain properly diagnosed. A foot and ankle surgeon is able to distinguish between all the possibilities and determine the underlying source of your heel pain.What Is Plantar Fasciitis? Plantar fasciitis is an inflammation of the band of tissue (the plantar fascia) that extends from the heel to the toes. In this condition, the fascia first becomes irritated and then inflamed, resulting in heel pain.
Causes
While heel pain has many causes, it is usually the result of faulty biomechanics (abnormalities in the way we walk). This can place too much stress on the heel bone and the soft tissues attached to it. The stress may also result from injury, or a bruise incurred while walking, running or jumping on hard surfaces; wearing poorly constructed footwear; or being significantly overweight. Systemic diseases such as arthritis and diabetes can also contribute to heel pain. A common cause of heel pain is the heel spur, a bony growth under the heel bone. There are no visible features on the heel, but a deep painful spot can be found in or around the middle of the sole of the heel (see diagram). Approximately 10 per cent of the population may have heel spurs without any pain. Heel spurs result from strain on the muscles of the foot. This may result from biomechanical imbalance, a condition occurring in many people. Both heel pain and heel spurs are frequently associated with an inflammation of the long band of tissue that connects the heel and the ball of the foot. The inflammation of this arch area is called plantar fasciitis. The inflammation may be aggravated by shoes that lack appropriate support, especially in the arch area, and by the chronic irritation that sometimes accompanies an athletic lifestyle.Excessive rolling in of the feet when walking. An inflamed bursa (bursitis), a small, irritated sack of fluid at the back of the heel. A neuroma (a nerve growth). Other soft-tissue growths. Heel bumps or ?pump bumps?, a bone enlargement at the back of the heel bone. Bruises or stress fractures to the heel bone.
Symptoms
Depending on the specific form of heel pain, symptoms may vary. Pain stemming from plantar fasciitis or heel spurs is particularly acute following periods of rest, whether it is after getting out of bed in the morning, or getting up after a long period of sitting. In many cases, pain subsides during activity as injured tissue adjusts to damage, but can return again with prolonged activity or when excessive pressure is applied to the affected area. Extended periods of activity and/or strain of the foot can increase pain and inflammation in the foot. In addition to pain, heel conditions can also generate swelling, bruising, and redness. The foot may also be hot to the touch, experience tingling, or numbness depending on the condition.
Diagnosis
A podiatrist (doctor who specializes in the evaluation and treatment of foot diseases) will carry out a physical examination, and ask pertinent questions about the pain. The doctor will also ask the patient how much walking and standing the patient does, what type of footwear is worn, and details of the his/her medical history. Often this is enough to make a diagnosis. Sometimes further diagnostic tests are needed, such as blood tests and imaging scans.
Non Surgical Treatment
Orthotics, by treating the cause of the problem, lead to the cure bette than 90% of the time. A small number of patients have waited so long that the plantar fascia has become thickened and filled with scar tissue and are not helped by ?conventional? means. Those are the patients that have, traditionally, required surgical treatment in which the plantar fascia is cut off the heel bone. Luckily, most surgery has been replaced by a relatively new mode of treatment, ESWT or Extracorporeal Shockwave Therapy. ESWT involves the application of multiple shockwaves to the diseased tendon or ligament and has an approximately 85 to 90% success rate. Keep in mind we are talking about this success rate in patients who are ?tough cases,? that is, already had the conventional treatment. The ESWT machines look like miniature renal lithtripsors (kidney stone crushers). There are virtually no side effects to ESWT other than the price as only about 30% of insurance companies are paying for it. They realize that it is less costly and safer than surgery but also know that many more people who would avoid surgery would have no problem getting ESWT so the volume of services would go up. You don?t have to live with painful heels.
Surgical Treatment
Although most patients with plantar fasciitis respond to non-surgical treatment, a small percentage of patients may require surgery. If, after several months of non-surgical treatment, you continue to have heel pain, surgery will be considered. Your foot and ankle surgeon will discuss the surgical options with you and determine which approach would be most beneficial for you. No matter what kind of treatment you undergo for plantar fasciitis, the underlying causes that led to this condition may remain. Therefore, you will need to continue with preventive measures. Wearing supportive shoes, stretching, and using custom orthotic devices are the mainstay of long-term treatment for plantar fasciitis.
heel spur exercises
Prevention
Preventing heel pain is crucial to avoid pain that can easily interrupt a busy or active lifestyle. Athletes can prevent damage by stretching the foot and calf both before and after an exercise routine. The plantar fascia ligament can be stretched by using a tennis ball or water bottle and rolling it across the bottom of the foot. With regular stretching, the stretching and flexibility of tissue through the foot can be significantly improved, helping to prevent damage and injury. Athletes should also ease into new or more difficult routines, allowing the plantar fascia and other tissue to become accustomed to the added stress and difficulty. Running up hills is also common among athletes in their routines. However, this activity should be reduced since it places an increased amount of stress on the plantar fascia and increases the risk of plantar fasciitis. Maintaining a healthy weight is also an essential heel pain prevention technique. Obesity brings additional weight and stress on the heel of the foot, causing damage and pain in the heel as well as in other areas of the foot.
Heel pain is most often caused by plantar fasciitis, a condition that is sometimes also called heel spur syndrome when a spur is present. Heel pain may also be due to other causes, such as a stress fracture, tendonitis, arthritis, nerve irritation, or, rarely, a cyst. Because there are several potential causes, it is important to have heel pain properly diagnosed. A foot and ankle surgeon is able to distinguish between all the possibilities and determine the underlying source of your heel pain.What Is Plantar Fasciitis? Plantar fasciitis is an inflammation of the band of tissue (the plantar fascia) that extends from the heel to the toes. In this condition, the fascia first becomes irritated and then inflamed, resulting in heel pain.
Causes
While heel pain has many causes, it is usually the result of faulty biomechanics (abnormalities in the way we walk). This can place too much stress on the heel bone and the soft tissues attached to it. The stress may also result from injury, or a bruise incurred while walking, running or jumping on hard surfaces; wearing poorly constructed footwear; or being significantly overweight. Systemic diseases such as arthritis and diabetes can also contribute to heel pain. A common cause of heel pain is the heel spur, a bony growth under the heel bone. There are no visible features on the heel, but a deep painful spot can be found in or around the middle of the sole of the heel (see diagram). Approximately 10 per cent of the population may have heel spurs without any pain. Heel spurs result from strain on the muscles of the foot. This may result from biomechanical imbalance, a condition occurring in many people. Both heel pain and heel spurs are frequently associated with an inflammation of the long band of tissue that connects the heel and the ball of the foot. The inflammation of this arch area is called plantar fasciitis. The inflammation may be aggravated by shoes that lack appropriate support, especially in the arch area, and by the chronic irritation that sometimes accompanies an athletic lifestyle.Excessive rolling in of the feet when walking. An inflamed bursa (bursitis), a small, irritated sack of fluid at the back of the heel. A neuroma (a nerve growth). Other soft-tissue growths. Heel bumps or ?pump bumps?, a bone enlargement at the back of the heel bone. Bruises or stress fractures to the heel bone.
Symptoms
Depending on the specific form of heel pain, symptoms may vary. Pain stemming from plantar fasciitis or heel spurs is particularly acute following periods of rest, whether it is after getting out of bed in the morning, or getting up after a long period of sitting. In many cases, pain subsides during activity as injured tissue adjusts to damage, but can return again with prolonged activity or when excessive pressure is applied to the affected area. Extended periods of activity and/or strain of the foot can increase pain and inflammation in the foot. In addition to pain, heel conditions can also generate swelling, bruising, and redness. The foot may also be hot to the touch, experience tingling, or numbness depending on the condition.
Diagnosis
A podiatrist (doctor who specializes in the evaluation and treatment of foot diseases) will carry out a physical examination, and ask pertinent questions about the pain. The doctor will also ask the patient how much walking and standing the patient does, what type of footwear is worn, and details of the his/her medical history. Often this is enough to make a diagnosis. Sometimes further diagnostic tests are needed, such as blood tests and imaging scans.
Non Surgical Treatment
Orthotics, by treating the cause of the problem, lead to the cure bette than 90% of the time. A small number of patients have waited so long that the plantar fascia has become thickened and filled with scar tissue and are not helped by ?conventional? means. Those are the patients that have, traditionally, required surgical treatment in which the plantar fascia is cut off the heel bone. Luckily, most surgery has been replaced by a relatively new mode of treatment, ESWT or Extracorporeal Shockwave Therapy. ESWT involves the application of multiple shockwaves to the diseased tendon or ligament and has an approximately 85 to 90% success rate. Keep in mind we are talking about this success rate in patients who are ?tough cases,? that is, already had the conventional treatment. The ESWT machines look like miniature renal lithtripsors (kidney stone crushers). There are virtually no side effects to ESWT other than the price as only about 30% of insurance companies are paying for it. They realize that it is less costly and safer than surgery but also know that many more people who would avoid surgery would have no problem getting ESWT so the volume of services would go up. You don?t have to live with painful heels.
Surgical Treatment
Although most patients with plantar fasciitis respond to non-surgical treatment, a small percentage of patients may require surgery. If, after several months of non-surgical treatment, you continue to have heel pain, surgery will be considered. Your foot and ankle surgeon will discuss the surgical options with you and determine which approach would be most beneficial for you. No matter what kind of treatment you undergo for plantar fasciitis, the underlying causes that led to this condition may remain. Therefore, you will need to continue with preventive measures. Wearing supportive shoes, stretching, and using custom orthotic devices are the mainstay of long-term treatment for plantar fasciitis.
heel spur exercises
Prevention
Preventing heel pain is crucial to avoid pain that can easily interrupt a busy or active lifestyle. Athletes can prevent damage by stretching the foot and calf both before and after an exercise routine. The plantar fascia ligament can be stretched by using a tennis ball or water bottle and rolling it across the bottom of the foot. With regular stretching, the stretching and flexibility of tissue through the foot can be significantly improved, helping to prevent damage and injury. Athletes should also ease into new or more difficult routines, allowing the plantar fascia and other tissue to become accustomed to the added stress and difficulty. Running up hills is also common among athletes in their routines. However, this activity should be reduced since it places an increased amount of stress on the plantar fascia and increases the risk of plantar fasciitis. Maintaining a healthy weight is also an essential heel pain prevention technique. Obesity brings additional weight and stress on the heel of the foot, causing damage and pain in the heel as well as in other areas of the foot.
Heel Lift For Functional Leg Length Discrepancy
Overview
Leg length discrepancy is an orthopaedic problem that usually appears in childhood, in which one's two legs are of unequal lengths. Often abbreviated as ?LLD,' leg length discrepancy may be caused by or associated with a number of other orthopaedic or medical conditions, but is generally treated in a similar fashion, regardless of cause and depending on severity. Leg length discrepancy is sometimes divided up into 'true LLD' and 'functional LLD.' Functional LLD occurs when the legs are actually equal in length, but some other condition, such as pelvic obliquity (a tilt in the position of the pelvis), creates the appearance of legs of different lengths.
Causes
Leg length discrepancies can be caused by poor alignment of the pelvis or simply because one leg is structurally longer than the other. Regardless of the reason, your body wants to be symmetrical and will do its best to compensate for the length difference. The greater the leg length difference, the earlier the symptoms will present themselves to the patient. Specific diagnoses that coincide with leg length discrepancy include: scoliosis, lumbar herniated discs, sacroiliitis, pelvic obiliquity, greater trochanteric bursitis, hip arthritis, piriformis syndrome, patellofemoral syndrome and foot pronation. Other potential causes could be due to an injury (such as a fracture), bone disease, bone tumors, congenital problems (present at birth) or from a neuromuscular problem.
Symptoms
The effects of limb length discrepancy vary from patient to patient, depending on the cause and size of the difference. Differences of 3 1/2 percent to 4 percent of the total length of the leg (about 4 cm or 1 2/3 inches in an average adult) may cause noticeable abnormalities when walking. These differences may require the patient to exert more effort to walk. There is controversy about the effect of limb length discrepancy on back pain. Some studies show that people with a limb length discrepancy have a greater incidence of low back pain and an increased susceptibility to injuries. Other studies do not support this finding.
Diagnosis
The only way to decipher between anatomical and functional leg length inequalities (you can have both) is by a physical measurement and series of biomechanical tests. It is actually a simple process and gets to the true cause of some runner?s chronic foot, knee, hip and back pain. After the muscles are tested and the legs are measured it may be necessary to get a special X-ray that measures both of your thighs (Femurs) and legs (Tibias). The X-ray is read by a medical radiologist who provides a report of the actual difference down to the micrometer leaving zero room for error. Once the difference in leg length is known, the solution becomes clear.
Non Surgical Treatment
A properly made foot orthotic can go a long way in substituting additional millimeters or centimeter on the deficient side. Additional full length inserts are added to the shorter side bringing the runner closer to symmetrical. Heel lifts do not work in runners because when you run you may land on your heel but the rest of the time you are on your forefoot then your toes pushing off. The right custom-made, biomechanical orthotic can address the underlying cause of your pain. Abnormal joint position, overpronation or foot rigidity can be addressed and the biomechanics normalized. San Diego Running Institute orthotics are custom molded to your foot and are designed with your specific body weight, leg length discrepancy, and activity in mind. The restoration of correct mechanical function takes the abnormal stress from the uneven side and allows the body to heal naturally.

shoe lifts for men's shoes
Surgical Treatment
Epiphysiodesis is a surgical option designed to slow down the growth of the long leg over a period of months to years. It is only used in growing children. The operation involves a general anaesthetic. Small incisions are made around the knee near the growth plates of the thigh bone and the shin bone. The growth plates are prevented from growing by the use of small screws and plates (?8 - plates?). The screws are buried beneath the skin and are not visible. Stitches are buried beneath the skin and do not need to be removed. The child is normally in hospital for 2-3 days. The child can weight bear immediately and return back to normal activity within a few weeks. Long term follow up is required to monitor the effects of the surgery. The timing of the surgery is based on the amount of growth predicted for the child. Therefore, this procedure can under- and over-correct the difference in leg length. Occasionally the screws have to be removed to allow growth to continue. This procedure can be used on one half of the growth plate to correct deformity in a limb e.g. knock-knees or bow legs. This is known as hemiepiphysiodesis.
Leg length discrepancy is an orthopaedic problem that usually appears in childhood, in which one's two legs are of unequal lengths. Often abbreviated as ?LLD,' leg length discrepancy may be caused by or associated with a number of other orthopaedic or medical conditions, but is generally treated in a similar fashion, regardless of cause and depending on severity. Leg length discrepancy is sometimes divided up into 'true LLD' and 'functional LLD.' Functional LLD occurs when the legs are actually equal in length, but some other condition, such as pelvic obliquity (a tilt in the position of the pelvis), creates the appearance of legs of different lengths.
Causes
Leg length discrepancies can be caused by poor alignment of the pelvis or simply because one leg is structurally longer than the other. Regardless of the reason, your body wants to be symmetrical and will do its best to compensate for the length difference. The greater the leg length difference, the earlier the symptoms will present themselves to the patient. Specific diagnoses that coincide with leg length discrepancy include: scoliosis, lumbar herniated discs, sacroiliitis, pelvic obiliquity, greater trochanteric bursitis, hip arthritis, piriformis syndrome, patellofemoral syndrome and foot pronation. Other potential causes could be due to an injury (such as a fracture), bone disease, bone tumors, congenital problems (present at birth) or from a neuromuscular problem.
Symptoms
The effects of limb length discrepancy vary from patient to patient, depending on the cause and size of the difference. Differences of 3 1/2 percent to 4 percent of the total length of the leg (about 4 cm or 1 2/3 inches in an average adult) may cause noticeable abnormalities when walking. These differences may require the patient to exert more effort to walk. There is controversy about the effect of limb length discrepancy on back pain. Some studies show that people with a limb length discrepancy have a greater incidence of low back pain and an increased susceptibility to injuries. Other studies do not support this finding.
Diagnosis
The only way to decipher between anatomical and functional leg length inequalities (you can have both) is by a physical measurement and series of biomechanical tests. It is actually a simple process and gets to the true cause of some runner?s chronic foot, knee, hip and back pain. After the muscles are tested and the legs are measured it may be necessary to get a special X-ray that measures both of your thighs (Femurs) and legs (Tibias). The X-ray is read by a medical radiologist who provides a report of the actual difference down to the micrometer leaving zero room for error. Once the difference in leg length is known, the solution becomes clear.
Non Surgical Treatment
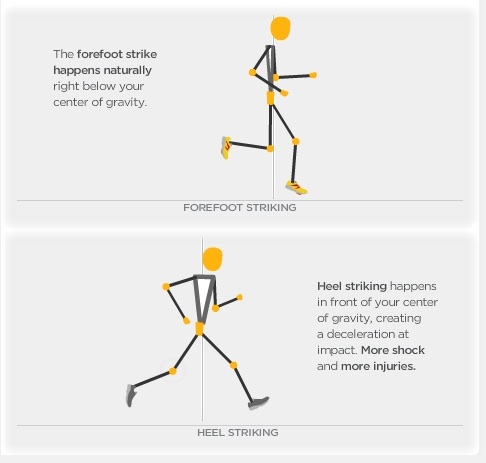
A properly made foot orthotic can go a long way in substituting additional millimeters or centimeter on the deficient side. Additional full length inserts are added to the shorter side bringing the runner closer to symmetrical. Heel lifts do not work in runners because when you run you may land on your heel but the rest of the time you are on your forefoot then your toes pushing off. The right custom-made, biomechanical orthotic can address the underlying cause of your pain. Abnormal joint position, overpronation or foot rigidity can be addressed and the biomechanics normalized. San Diego Running Institute orthotics are custom molded to your foot and are designed with your specific body weight, leg length discrepancy, and activity in mind. The restoration of correct mechanical function takes the abnormal stress from the uneven side and allows the body to heal naturally.
shoe lifts for men's shoes
Surgical Treatment
Epiphysiodesis is a surgical option designed to slow down the growth of the long leg over a period of months to years. It is only used in growing children. The operation involves a general anaesthetic. Small incisions are made around the knee near the growth plates of the thigh bone and the shin bone. The growth plates are prevented from growing by the use of small screws and plates (?8 - plates?). The screws are buried beneath the skin and are not visible. Stitches are buried beneath the skin and do not need to be removed. The child is normally in hospital for 2-3 days. The child can weight bear immediately and return back to normal activity within a few weeks. Long term follow up is required to monitor the effects of the surgery. The timing of the surgery is based on the amount of growth predicted for the child. Therefore, this procedure can under- and over-correct the difference in leg length. Occasionally the screws have to be removed to allow growth to continue. This procedure can be used on one half of the growth plate to correct deformity in a limb e.g. knock-knees or bow legs. This is known as hemiepiphysiodesis.
Leg Length Discrepancy After Knee Surgery
Overview
Large leg length inequalities can be treated by staged lengthenings or by simultaneous ipsilateral femoral and tibial lengthenings. Additionally, lengthenings can be combined with appropriately timed epiphysiodesis in an effort to produce leg length equality. Staged lengthenings are often used for congenital deficiencies such as fibular hemimelia, in which 15 cm or more may be needed to produce leg length equality. We typically plan for the final lengthening to be completed by age 13 or 14 years, and allow at least 3 years between lengthenings. Lengthening of both the tibia and femur simultaneously requires aggressive therapy and treatment of soft tissue contractures. Curran et al[57] reported the need for surgical release of soft tissue contractures in 3 of 8 patients treated with simultaneous ipsilateral femoral and tibial lengthenings. Lengthening over an IM nail can be done in an effort to decrease the amount of time the fixator needs to be worn and to prevent angular malalignment. This technique requires that the patient be skeletally mature and it carries a higher risk of osteomyelitis (up to 15%). Additionally, if premature consolidation occurs, a repeat corticotomy is more difficult.
Causes
The causes of LLD are many, including a previous injury, bone infection, bone diseases (dysplasias), inflammation (arthritis) and neurologic conditions. Previously broken bones may cause LLD by healing in a shortened position, especially if the bone was broken in many pieces (comminuted) or if skin and muscle tissue around the bone were severely injured and exposed (open fracture). Broken bones in children sometimes grow faster for several years after healing, causing the injured bone to become longer. Also, a break in a child?s bone through a growth center (located near the ends of the bone) may cause slower growth, resulting in a shorter extremity. Bone infections that occur in children while they are growing may cause a significant LLD, especially during infancy. Bone diseases may cause LLD, as well; examples are neurofibromatosis, multiple hereditary exostoses and Ollier disease. Inflammation of joints during growth may cause unequal extremity length. One example is juvenile rheumatoid arthritis. Osteoarthritis, the joint degeneration that occurs in adults, very rarely causes a significant LLD.
Symptoms
Faulty feet and ankle structure profoundly affect leg length and pelvic positioning. The most common asymmetrical foot position is the pronated foot. Sensory receptors embedded on the bottom of the foot alert the brain to the slightest weight shift. Since the brain is always trying to maintain pelvic balance, when presented with a long left leg, it attempts to adapt to the altered weight shift by dropping the left medial arch (shortening the long leg) and supinating the right arch to lengthen the short leg.1 Left unchecked, excessive foot pronation will internally rotate the left lower extremity, causing excessive strain to the lateral meniscus and medial collateral knee ligaments. Conversely, excessive supination tends to externally rotate the leg and thigh, creating opposite knee, hip and pelvic distortions.
Diagnosis
Leg length discrepancy may be diagnosed during infancy or later in childhood, depending on the cause. Conditions such as hemihypertrophy or hemiatrophy are often diagnosed following standard newborn or infant examinations by a pediatrician, or anatomical asymmetries may be noticed by a child's parents. For young children with hemihypertophy as the cause of their LLD, it is important that they receive an abdominal ultrasound of the kidneys to insure that Wilm's tumor, which can lead to hypertrophy in the leg on the same side, is not present. In older children, LLD is frequently first suspected due to the emergence of a progressive limp, warranting a referral to a pediatric orthopaedic surgeon. The standard workup for LLD is a thorough physical examination, including a series of measurements of the different portions of the lower extremities with the child in various positions, such as sitting and standing. The orthopaedic surgeon will observe the child while walking and performing other simple movements or tasks, such as stepping onto a block. In addition, a number of x-rays of the legs will be taken, so as to make a definitive diagnosis and to assist with identification of the possible etiology (cause) of LLD. Orthopaedic surgeons will compare x-rays of the two legs to the child's age, so as to assess his/her skeletal age and to obtain a baseline for the possibility of excessive growth rate as a cause. A growth chart, which compares leg length to skeletal age, is a simple but essential tool used over time to track the progress of the condition, both before and after treatment. Occasionally, a CT scan or MRI is required to further investigate suspected causes or to get more sophisticated radiological pictures of bone or soft tissue.
Non Surgical Treatment
Non-surgical treatment can be effective. A shoe lift may be recommended if the leg length difference is less than 1 inch. More significant leg length discrepancies may require a surgical procedure. In children, surgical procedures are available to help make leg lengths more equal.

what happens if one leg is shorter than the other?
Surgical Treatment
The type of surgery depends on the type of problem. Outpatient procedures may be used to alter the growth of the limb. This is often done through small incisions. If an outpatient procedure is done, your child can continue with most regular activities. Other times, surgery may be very involved and require the use of an external device that is attached to the limb with pins and wires. This device may be left on for months to correct the deformity or lengthen the leg. If this type of surgery is required, your child will be making weekly visits to Cincinnati Children's.
Large leg length inequalities can be treated by staged lengthenings or by simultaneous ipsilateral femoral and tibial lengthenings. Additionally, lengthenings can be combined with appropriately timed epiphysiodesis in an effort to produce leg length equality. Staged lengthenings are often used for congenital deficiencies such as fibular hemimelia, in which 15 cm or more may be needed to produce leg length equality. We typically plan for the final lengthening to be completed by age 13 or 14 years, and allow at least 3 years between lengthenings. Lengthening of both the tibia and femur simultaneously requires aggressive therapy and treatment of soft tissue contractures. Curran et al[57] reported the need for surgical release of soft tissue contractures in 3 of 8 patients treated with simultaneous ipsilateral femoral and tibial lengthenings. Lengthening over an IM nail can be done in an effort to decrease the amount of time the fixator needs to be worn and to prevent angular malalignment. This technique requires that the patient be skeletally mature and it carries a higher risk of osteomyelitis (up to 15%). Additionally, if premature consolidation occurs, a repeat corticotomy is more difficult.
Causes
The causes of LLD are many, including a previous injury, bone infection, bone diseases (dysplasias), inflammation (arthritis) and neurologic conditions. Previously broken bones may cause LLD by healing in a shortened position, especially if the bone was broken in many pieces (comminuted) or if skin and muscle tissue around the bone were severely injured and exposed (open fracture). Broken bones in children sometimes grow faster for several years after healing, causing the injured bone to become longer. Also, a break in a child?s bone through a growth center (located near the ends of the bone) may cause slower growth, resulting in a shorter extremity. Bone infections that occur in children while they are growing may cause a significant LLD, especially during infancy. Bone diseases may cause LLD, as well; examples are neurofibromatosis, multiple hereditary exostoses and Ollier disease. Inflammation of joints during growth may cause unequal extremity length. One example is juvenile rheumatoid arthritis. Osteoarthritis, the joint degeneration that occurs in adults, very rarely causes a significant LLD.
Symptoms
Faulty feet and ankle structure profoundly affect leg length and pelvic positioning. The most common asymmetrical foot position is the pronated foot. Sensory receptors embedded on the bottom of the foot alert the brain to the slightest weight shift. Since the brain is always trying to maintain pelvic balance, when presented with a long left leg, it attempts to adapt to the altered weight shift by dropping the left medial arch (shortening the long leg) and supinating the right arch to lengthen the short leg.1 Left unchecked, excessive foot pronation will internally rotate the left lower extremity, causing excessive strain to the lateral meniscus and medial collateral knee ligaments. Conversely, excessive supination tends to externally rotate the leg and thigh, creating opposite knee, hip and pelvic distortions.
Diagnosis
Leg length discrepancy may be diagnosed during infancy or later in childhood, depending on the cause. Conditions such as hemihypertrophy or hemiatrophy are often diagnosed following standard newborn or infant examinations by a pediatrician, or anatomical asymmetries may be noticed by a child's parents. For young children with hemihypertophy as the cause of their LLD, it is important that they receive an abdominal ultrasound of the kidneys to insure that Wilm's tumor, which can lead to hypertrophy in the leg on the same side, is not present. In older children, LLD is frequently first suspected due to the emergence of a progressive limp, warranting a referral to a pediatric orthopaedic surgeon. The standard workup for LLD is a thorough physical examination, including a series of measurements of the different portions of the lower extremities with the child in various positions, such as sitting and standing. The orthopaedic surgeon will observe the child while walking and performing other simple movements or tasks, such as stepping onto a block. In addition, a number of x-rays of the legs will be taken, so as to make a definitive diagnosis and to assist with identification of the possible etiology (cause) of LLD. Orthopaedic surgeons will compare x-rays of the two legs to the child's age, so as to assess his/her skeletal age and to obtain a baseline for the possibility of excessive growth rate as a cause. A growth chart, which compares leg length to skeletal age, is a simple but essential tool used over time to track the progress of the condition, both before and after treatment. Occasionally, a CT scan or MRI is required to further investigate suspected causes or to get more sophisticated radiological pictures of bone or soft tissue.
Non Surgical Treatment
Non-surgical treatment can be effective. A shoe lift may be recommended if the leg length difference is less than 1 inch. More significant leg length discrepancies may require a surgical procedure. In children, surgical procedures are available to help make leg lengths more equal.
what happens if one leg is shorter than the other?
Surgical Treatment
The type of surgery depends on the type of problem. Outpatient procedures may be used to alter the growth of the limb. This is often done through small incisions. If an outpatient procedure is done, your child can continue with most regular activities. Other times, surgery may be very involved and require the use of an external device that is attached to the limb with pins and wires. This device may be left on for months to correct the deformity or lengthen the leg. If this type of surgery is required, your child will be making weekly visits to Cincinnati Children's.
What Is Mortons Neuroma
Overview
 A Morton's neuroma is a benign (noncancerous) swelling along a nerve in the foot that carries sensations from the toes. The reason the nerve starts to swell is unknown. But once swelling begins, the nearby bones and ligaments put pressure on the nerve, causing more irritation and inflammation. This produces burning pain, numbness, tingling and other abnormal sensations in the toes. A Morton's neuroma also is called an interdigital neuroma, intermetatarsal neuroma or a forefoot neuroma.
A Morton's neuroma is a benign (noncancerous) swelling along a nerve in the foot that carries sensations from the toes. The reason the nerve starts to swell is unknown. But once swelling begins, the nearby bones and ligaments put pressure on the nerve, causing more irritation and inflammation. This produces burning pain, numbness, tingling and other abnormal sensations in the toes. A Morton's neuroma also is called an interdigital neuroma, intermetatarsal neuroma or a forefoot neuroma.
Causes
Morton's neuroma develops for several reasons. The primary reason is wearing narrow toe-box shoes, which compress the metatarsal heads. Certain anatomical factors also make nerve compression more likely with the narrow toe box shoes. In some people fibers, the medial and lateral plantar nerves converge close to the heads of the third and fourth metatarsals. This junction creates a larger nerve structure between the metatarsal heads making it more vulnerable to compression.
Symptoms
Morton's neuroma can cause a very painful burning or sharp pain in your foot that feels worse when you walk. It may feel like a small lump inside the ball of your foot. It is usually between the third and fourth toes, but it can also be between other toes.
Diagnosis
The doctor will ask about your symptoms and medical history. A physical exam will be done. Initial diagnosis of Morton's neuroma is based on your description of the type and location of pain and discomfort in the foot. The diagnosis will be confirmed by a physical exam of the foot, including checking for mechanical abnormalities in the foot, squeezing the side of the foot, which will usually cause pain when Morton's neuroma is present. Examination of your shoes to check for excess wear in parts of the shoe, check to see whether the shoes are too tight. Imaging tests evaluate the foot and surrounding structures. This may be done with X-ray, MRI scan, Ultrasound. Injections of local anesthetic can also be used for diagnosis.
Non Surgical Treatment
Pain is the main reason that you seek treatment for a neuroma. Analgesics may help. Inflammation it best eased via ice therapy and techniques or exercises that deload the inflammed structures. Anti-inflammatory medications may help. Your physiotherapist will use an array of treatment tools to reduce your pain and inflammation. These include: ice, electrotherapy, acupuncture, deloading taping techniques, soft tissue massage and orthotics to offload the irritated nerve. One of the biggest factors in relieving pain may be changing or modifying your footwear. This may mean adding felt, foam or gel products to your shoe to help offload the area, or looking at avoiding tight fitting heels or shoes.
Surgical Treatment
When medications or other treatments do not work, podiatric surgery may be required. The most common surgical procedure for treating Morton?s neuroma is a neurectomy, in which part of the nerve tissue is removed. Although this procedure effectively removes the original neuroma, sometimes scar tissue known as a stump neuroma forms at the site of the incision. This may result in tingling, numbness, or pain following surgery. Surgery is effective in relieving or reducing symptoms for Morton?s neuroma patients in about 75% to 85% of all cases. Occasionally, minimally invasive radio frequency ablation is also used to treat Morton's neuroma.
A Morton's neuroma is a benign (noncancerous) swelling along a nerve in the foot that carries sensations from the toes. The reason the nerve starts to swell is unknown. But once swelling begins, the nearby bones and ligaments put pressure on the nerve, causing more irritation and inflammation. This produces burning pain, numbness, tingling and other abnormal sensations in the toes. A Morton's neuroma also is called an interdigital neuroma, intermetatarsal neuroma or a forefoot neuroma.Causes
Morton's neuroma develops for several reasons. The primary reason is wearing narrow toe-box shoes, which compress the metatarsal heads. Certain anatomical factors also make nerve compression more likely with the narrow toe box shoes. In some people fibers, the medial and lateral plantar nerves converge close to the heads of the third and fourth metatarsals. This junction creates a larger nerve structure between the metatarsal heads making it more vulnerable to compression.
Symptoms
Morton's neuroma can cause a very painful burning or sharp pain in your foot that feels worse when you walk. It may feel like a small lump inside the ball of your foot. It is usually between the third and fourth toes, but it can also be between other toes.
Diagnosis
The doctor will ask about your symptoms and medical history. A physical exam will be done. Initial diagnosis of Morton's neuroma is based on your description of the type and location of pain and discomfort in the foot. The diagnosis will be confirmed by a physical exam of the foot, including checking for mechanical abnormalities in the foot, squeezing the side of the foot, which will usually cause pain when Morton's neuroma is present. Examination of your shoes to check for excess wear in parts of the shoe, check to see whether the shoes are too tight. Imaging tests evaluate the foot and surrounding structures. This may be done with X-ray, MRI scan, Ultrasound. Injections of local anesthetic can also be used for diagnosis.
Non Surgical Treatment
Pain is the main reason that you seek treatment for a neuroma. Analgesics may help. Inflammation it best eased via ice therapy and techniques or exercises that deload the inflammed structures. Anti-inflammatory medications may help. Your physiotherapist will use an array of treatment tools to reduce your pain and inflammation. These include: ice, electrotherapy, acupuncture, deloading taping techniques, soft tissue massage and orthotics to offload the irritated nerve. One of the biggest factors in relieving pain may be changing or modifying your footwear. This may mean adding felt, foam or gel products to your shoe to help offload the area, or looking at avoiding tight fitting heels or shoes.
Surgical Treatment
When medications or other treatments do not work, podiatric surgery may be required. The most common surgical procedure for treating Morton?s neuroma is a neurectomy, in which part of the nerve tissue is removed. Although this procedure effectively removes the original neuroma, sometimes scar tissue known as a stump neuroma forms at the site of the incision. This may result in tingling, numbness, or pain following surgery. Surgery is effective in relieving or reducing symptoms for Morton?s neuroma patients in about 75% to 85% of all cases. Occasionally, minimally invasive radio frequency ablation is also used to treat Morton's neuroma.
For Leg Length Imbalances Chiropodists Prefer Shoe Lifts
There are not one but two unique variations of leg length discrepancies, congenital and acquired. Congenital implies you are born with it. One leg is anatomically shorter than the other. As a result of developmental periods of aging, the human brain picks up on the stride pattern and identifies some variance. Your body usually adapts by dipping one shoulder to the "short" side. A difference of less than a quarter inch isn't blatantly excessive, does not need Shoe Lifts to compensate and mostly does not have a serious effect over a lifetime.

Leg length inequality goes typically undiscovered on a daily basis, yet this issue is very easily remedied, and can eliminate a number of instances of chronic back pain.
Therapy for leg length inequality commonly consists of Shoe Lifts. These are generally low cost, usually being below twenty dollars, in comparison to a custom orthotic of $200 or higher. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Mid back pain is the most common ailment afflicting men and women today. Over 80 million people experience back pain at some point in their life. It is a problem that costs companies huge amounts of money year after year due to time lost and output. Innovative and improved treatment solutions are continually sought after in the hope of decreasing the economical influence this issue causes.

People from all corners of the world suffer the pain of foot ache as a result of leg length discrepancy. In most of these cases Shoe Lifts can be of beneficial. The lifts are capable of reducing any discomfort and pain in the feet. Shoe Lifts are recommended by many professional orthopaedic physicians.
So that they can support the body in a well-balanced manner, your feet have got a very important job to play. Despite that, it can be the most neglected region in the human body. Some people have flat-feet meaning there may be unequal force placed on the feet. This causes other areas of the body such as knees, ankles and backs to be impacted too. Shoe Lifts make sure that the right posture and balance are restored.
Leg length inequality goes typically undiscovered on a daily basis, yet this issue is very easily remedied, and can eliminate a number of instances of chronic back pain.
Therapy for leg length inequality commonly consists of Shoe Lifts. These are generally low cost, usually being below twenty dollars, in comparison to a custom orthotic of $200 or higher. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Mid back pain is the most common ailment afflicting men and women today. Over 80 million people experience back pain at some point in their life. It is a problem that costs companies huge amounts of money year after year due to time lost and output. Innovative and improved treatment solutions are continually sought after in the hope of decreasing the economical influence this issue causes.
People from all corners of the world suffer the pain of foot ache as a result of leg length discrepancy. In most of these cases Shoe Lifts can be of beneficial. The lifts are capable of reducing any discomfort and pain in the feet. Shoe Lifts are recommended by many professional orthopaedic physicians.
So that they can support the body in a well-balanced manner, your feet have got a very important job to play. Despite that, it can be the most neglected region in the human body. Some people have flat-feet meaning there may be unequal force placed on the feet. This causes other areas of the body such as knees, ankles and backs to be impacted too. Shoe Lifts make sure that the right posture and balance are restored.
What Is The Most Suitable Treatment For Heel Spur

Overview
Heel spurs are a common reason for people to visit their podiatrist serving Scottsdale. These small calcium deposits can cause major pain, but treatments are available to relieve your symptoms. Heel spurs grow along the plantar fascia and create a sensation similar to that of a pebble being stuck in your shoe. Your podiatrist will use a physical exam plus X-rays to determine if a heel spur is the cause of your foot pain before beginning treatment. If you do have a heel spur, your podiatrist may recommend a cortisone injection to ease inflammation. Other techniques, such as stretching the calf muscles, treating the heel with ice, and wearing a custom orthotic may also provide relief from the discomfort of a heel spur.
Causes
Bone spurs form in the feet in response to tight ligaments, to activities such as dancing and running that put stress on the feet, and to pressure from being overweight or from poorly fitting shoes. For example, the long ligament on the bottom of the foot (plantar fascia) can become stressed or tight and pull on the heel, causing the ligament to become inflamed (plantar fasciitis). As the bone tries to mend itself, a bone spur can form on the bottom of the heel (known as a ?heel spur?). Pressure at the back of the heel from frequently wearing shoes that are too tight can cause a bone spur on the back of the heel. This is sometimes called a ?pump bump,? because it is often seen in women who wear high heels.

Symptoms
It is important to be aware that heel spurs may or may not cause symptoms. Symptoms are usually related to the plantar fasciitis. You may experience significant pain and it may be worse in the morning when you first wake up or during certain physical activities such as, walking, jogging, or running.
Diagnosis
Heel spurs and plantar fasciitis is usually diagnosed by your physiotherapist or sports doctor based on your symptoms, history and clinical examination. After confirming your heel spur or plantar fasciitis they will investigate WHY you are likely to be predisposed to heel spurs and develop a treatment plan to decrease your chance of future bouts. X-rays will show calcification or bone within the plantar fascia or at its insertion into the calcaneus. This is known as a calcaneal or heel spur. Ultrasound scans and MRI are used to identify any plantar fasciitis tears, inflammation or calcification. Pathology tests may identify spondyloarthritis, which can cause symptoms similar to plantar fasciitis.
Non Surgical Treatment
Podiatric Care for heel spur syndrome may involve keeping the fascia stretched out by performing exercises. Your doctor may also suggest for you to be seen by a physical therapist. You probably will be advised on the best shoes to wear or some inserts for your shoes. Your podiatrist may suggest that a custom made orthotic be made to allow your foot to function in the most ideal way especially if you have excessive pronation. A heel lift may be used if you have a leg length discrepancy. Medical treatment may include anti-inflammatory oral medications or an injection of medication and local anesthetic to reduce the swelling and decrease pain. If a bursitis is present the medication may greatly improve the symptoms. Your podiatric physician may also recommend a surgical procedure to actually fix the structural problem of your foot.
Surgical Treatment
Heel spur surgery should only be considered after less invasive treatment methods have been explored and ruled insufficient. The traditional surgical approach to treating heel spurs requires a scalpel cut to the bottom of the food which allows the surgeon to access the bone spur. Endoscopic plantar fasciotomies (EPF) involve one or two small incisions in the foot which allow the surgeon to access and operate on the bone spur endoscopically. Taking a surgical approach to heel spur treatment is a topic to explore with a foot and ankle specialist.
Prevention
You can prevent heel spurs by wearing well-fitting shoes with shock-absorbent soles, rigid shanks, and supportive heel counters; choosing appropriate shoes for each physical activity; warming up and doing stretching exercises before each activity; and pacing yourself during the activities. Avoid wearing shoes with excessive wear on the heels and soles. If you are overweight, losing weight may also help prevent heel spurs.